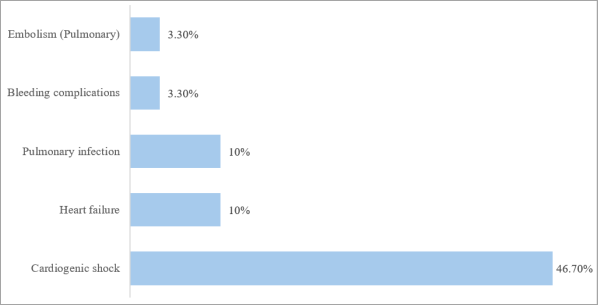
Acute Coronary Syndrome (ACS) significantly contributes to cardiovascular mortality worldwide, with an increasing prevalence in Africa due to rising cardiovascular risk factors. Despite advances in reperfusion therapies like percutaneous coronary intervention (PCI), many African countries, including Senegal, face substantial barriers to optimal care. This study aimed to assess in-hospital mortality among ACS patients undergoing coronary angiography in Dakar, Senegal, and to describe clinical features associated with mortality. We conducted a retrospective, multicenter, cross-sectional study involving patients hospitalized with ACS who underwent coronary angiography between January 2020 and June 2023 in three tertiary cardiology centers in Dakar. Demographic data, clinical presentation, cardiovascular risk factors, angiographic findings, and therapeutic interventions were collected. Statistical analysis included descriptive statistics and bivariate comparisons, with significance defined at p<0.05. Out of 2573 ACS patients undergoing coronary angiography, 30 died, resulting in an in-hospital mortality rate of 1.16%. The mean age was 61.2 ± 10.8 years, predominantly male (76.7%). Hypertension (53.3%) and sedentary lifestyle (83.3%) were common risk factors. Most patients presented with atypical chest pain (76.7%) and delayed hospital admission beyond 12 hours (43.3%). STEMI accounted for 70% of cases, with the left anterior descending artery frequently involved (80%). PCI using drug-eluting stents was performed in 56.7% of deceased patients. Cardiogenic shock was the leading complication (46.7%). In-hospital mortality following coronary angiography for ACS in urban Senegal is relatively low but delayed presentations and atypical symptoms remain significant barriers. Enhanced public awareness, reduced delays to intervention, and overcoming socioeconomic obstacles are essential to improve outcomes.
| Published in | Cardiology and Cardiovascular Research (Volume 9, Issue 2) |
| DOI | 10.11648/j.ccr.20250902.12 |
| Page(s) | 47-53 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Acute Coronary Syndrome, Percutaneous Coronary Intervention, In-hospital Mortality, Sub-Saharan Africa
Characteristic | Percentage (%) or Mean ± SD |
|---|---|
Sociodemographic Variables | |
Age (years) | 61.4 ± 12.3 |
Male Gender | 76.7% |
Sedentary Lifestyle | 83.3% |
Cardiovascular Risk Factors | |
Hypertension | 53.3% |
Diabetes mellitus | 46.7% |
Dyslipidemia | 20% |
Active smoking | 23.3% |
Obesity | 3.3% |
Clinical Presentation | |
Typical chest pain | 23.3% |
Atypical chest pain | 76.7% |
Killip classification ≥ II | 46.7% |
Admission delay (>12 hours) | 43.3% |
Coronary Angiography Findings | |
Radial approach | 76.7% |
Femoral approach | 23.3% |
Left Anterior Descending artery lesions | 80% |
Right coronary artery lesions | 53.3% |
Multivessel coronary disease | 60% |
Interventional Procedures | |
Angioplasty performed | 56.7% |
Drug-eluting stent used | 100% |
Thrombolysis attempted | 30% |
Medications | |
Aspirin | 86.7% |
Clopidogrel | 86.7% |
Statins | 86.7% |
Beta-blockers | 66.7% |
ACE inhibitors/ARBs | 63.3% |
Low molecular weight heparin | 83.3% |
Outcomes | |
In-hospital mortality | 1.16% |
Length of hospital stay (days) | 6.2 ± 4.7 days |
Variables | Angioplasty (n=17) | No Angioplasty (n=13) | p-value |
|---|---|---|---|
Age (years) Mean ± SD | 59.2 ± 10.1 | 63.8 ± 14.2 | 0.331 |
Male gender n (%) | 13 (76.5%) | 10 (76.9%) | 0.978 |
Cardiovascular risk factors | |||
Hypertension n (%) | 7 (50.0%) | 7 (50.0%) | 0.491 |
Diabetes mellitus n (%) | 10 (71.4%) | 4 (28.6%) | 0.127 |
Smoking n (%) | 4 (57.1%) | 3 (42.9%) | 0.660 |
Chest pain type | |||
Typical n (%) | 4 (57.1%) | 3 (42.9%) | 0.631 |
Atypical n (%) | 13 (59.1%) | 9 (40.9%) | 0.631 |
Admission delay | |||
≤12 hours n (%) | 10 (76.9%) | 3 (23.1%) | 0.072 |
>12 hours n (%) | 6 (42.9%) | 8 (57.1%) | 0.072 |
ACS Type | |||
STEMI n (%) | 13 (61.9%) | 8 (38.1%) | 0.204 |
NSTEMI n (%) | 4 (30.8%) | 5 (69.2%) | 0.310 |
ECG territory | |||
Inferior STEMI n (%) | 2 (22.2%) | 7 (77.8%) | 0.018 |
Anterior STEMI n (%) | 7 (100%) | 0 (0%) | 0.010 |
ECG territory | |||
Left anterior descending artery n (%) | 15 (62.5%) | 9 (37.5%) | 0.204 |
Right coronary artery n (%) | 7 (43.8%) | 9 (56.2%) | 0.127 |
Triple-vessel disease n (%) | 7 (43.8%) | 9 (56.2%) | 0.127 |
Complications during hospitalization | |||
Cardiogenic shock n (%) | 7 (50.0%) | 7 (50.0%) | 0.491 |
Heart failure n (%) | 1 (33.3%) | 2 (66.7%) | 0.402 |
Laboratory parameters | |||
Hemoglobin ≤10 g/dL n (%) | 4 (57.1%) | 3 (42.9%) | 0.546 |
Glomerular filtration rate <60 ml/min n (%) | 6 (60.0%) | 4 (40.0%) | 0.402 |
ACE | Angiotensin Conversion Enzyme |
ACS | Acute Coronary Syndrome |
AMI | Acute Myocardial Infarction |
ARBs | Angiotensin Receptor Blockers |
BMI | Body Mass Index |
CABG | Coronary Artery Bypass Grafting |
CAD | Coronary Artery Disease |
CK-MB | Creatin Kinase-MB |
CRP | C-reactive Protein |
ECG | Electrocardiogramm |
HDL-C | High Density Lipoprotein-C |
IU | International Unit |
IV | Intravenous |
LDL-C | Low Density Lipoprotein-C |
LVEF | Left Ventricular Ejection Fraction |
MDRD | Modification of Diet in Renal Disease |
NSTEMI | Non-ST Elevation Myocardial Infarction |
PCI | Percutaneous Coronary Intervention |
RACE-Nigeria | Registry for Acute Coronary Events in Nigeria |
SD | Standard Deviation |
SPSS | Statistical Package for the Social Sciences |
SSA | Sub-Saharan Africa |
STEMI | ST-elevation Myocardial Infarction |
| [1] | Yao H, Ekou A, Niamkey T, Gan SH, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub-Saharan Africa: A 10-Year Systematic Review. Journal of the American Heart Association. 2022 Jan 4; 11(1). |
| [2] | Shehu MN, Adamu UG, Ojji DB, Ogah OS, Sani MU. The Pandemic of Coronary Artery Disease in the Sub-Saharan Africa: What Clinicians Need to Know. Curr Atheroscler Rep. 2023 Sep; 25(9): 571–8. |
| [3] | Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016 Jul; 4(13): 256. |
| [4] | De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time Delay to Treatment and Mortality in Primary Angioplasty for Acute Myocardial Infarction. Circulation. 2004 Mar 16; 109(10): 1223–5. |
| [5] | Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. European Heart Journal. 2023 Oct 12; 44(38): 3720–826. |
| [6] | Rao SV, O’Donoghue ML, Ruel M, Rab T, Tamis-Holland JE, Alexander JH, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025 Feb 27; CIR. 0000000000001309. |
| [7] | Rao A, Kardouh Y, Darda S, Desai D, Devireddy L, Lalonde T, et al. Impact of the prehospital ECG on door‐to‐balloon time in ST elevation myocardial infarction. Cathet Cardio Intervent. 2010 Feb; 75(2): 174–8. |
| [8] | Rathore SS, Curtis JP, Chen J, Wang Y, Nallamothu BK, Epstein AJ, et al. Association of door-to-balloon time and mortality in patients admitted to hospital with ST elevation myocardial infarction: national cohort study. BMJ. 2009 May 19; 338(may19 1): b1807–b1807. |
| [9] | McNamara RL, Wang Y, Herrin J, Curtis JP, Bradley EH, Magid DJ, et al. Effect of Door-to-Balloon Time on Mortality in Patients With ST-Segment Elevation Myocardial Infarction. JACC. 2006; 47(11): 2180–6. |
| [10] | Moustaghfir A, Haddak M, Mechmeche R. Management of acute coronary syndromes in Maghreb countries: The ACCESS (ACute Coronary Events – a multinational Survey of current management Strategies) registry. Archives of Cardiovascular Diseases. 2012 Nov; 105(11): 566–77. |
| [11] | Stassen W, Wallis L, Lambert C, Castren M, Kurland L. Percutaneous coronary intervention still not accessible for many South Africans. African Journal of Emergency Medicine. 2017 Sep 1; 7(3): 105–7. |
| [12] | Cilliers JCD, Joubert L, Beyers B, Ngarande E, Herbst P, Doubell A, et al. The incidence and outcomes of high-risk acute coronary syndromes in Western Cape Province, South Africa: A prospective cohort study. S Afr Med J. 2023 Apr 12; 113(5): 25–9. |
| [13] | Fanta K, Daba FB, Asefa ET, Melaku T, Chelkeba L, Fekadu G, et al. Management and 30-Day Mortality of Acute Coronary Syndrome in a Resource-Limited Setting: Insight From Ethiopia. A Prospective Cohort Study. Front Cardiovasc Med. 2021; 8: 707700. |
| [14] | Varwani MH, Jeilan M, Ngunga M, Barasa A. Outcomes in patients with acute coronary syndrome in a referral hospital in sub-Saharan Africa. Cardiovasc J Afr. 2019 Feb 23; 30(1): 29–33. |
| [15] | Bahiru E, Temu T, Gitura B, Farquhar C, Huffman MD, Bukachi F. Presentation, management and outcomes of acute coronary syndrome: a registry study from Kenyatta National Hospital in Nairobi, Kenya. Cardiovasc J Afr. 2018 Aug 23; 29(4): 225–30. |
| [16] | Lim GB. Acute coronary syndromes: Reduced mortality from MI in Denmark, England, and Poland. Nat Rev Cardiol. 2012 Feb 21; 9(4): 186. |
| [17] | Adem F, Abdi S, Amare F, Mohammed MA. In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis. SAGE Open Medicine. 2023 Jan 1; 11: 20503121221143646. |
| [18] | Yao H, Ekou A, Hadéou A, N’Djessan JJ, Kouamé I, N’Guetta R. Medium and long-term follow-up after ST-segment elevation myocardial infarction in a sub-Saharan Africa population: a prospective cohort study. BMC Cardiovasc Disord. 2019 Dec; 19(1): 65. |
| [19] | Yao H, Ekou A, Niamkey T, Touré C, Guenancia C, Kouamé I, et al. Prognostic value of admission hyperglycaemia in black Africans with acute coronary syndromes: a crosssectional study. CVJA. 2020 Dec 15; 31(6): 39–44. |
| [20] | Ekou A, Kipenge R, Yao H, Ehouman E, Touré C, Vy L, et al. Thirty-day and one-year outcomes and predictors of mortality following acute myocardial infarction in Côte d’Ivoire: Data from the REACTIV survey. Archives of Cardiovascular Diseases. 2024 Jan; 117(1): S21–2. |
| [21] | Isezuo S, Sani MU, Talle A, Johnson A, Adeoye AM, Ulgen MS, et al. Registry for Acute Coronary Events in Nigeria (RACE-Nigeria): Clinical Characterization, Management, and Outcome. J Am Heart Assoc. 2022 Jan 4; 11(1): e020244. |
| [22] | El-Menyar A, Zubaid M, Sulaiman K, AlMahmeed W, Singh R, Alsheikh-Ali AA, et al. Atypical presentation of acute coronary syndrome: A significant independent predictor of in-hospital mortality. Journal of Cardiology. 2011 Mar 1; 57(2): 165–71. |
APA Style
Gaye, N. D., Ngaide, A. A., Ngoulla, P., Mingou, J., Dioum, M., et al. (2025). In-Hospital Mortality of Acute Coronary Syndromes Undergoing Coronary Angiography: A Multicenter Study in Dakar, Senegal. Cardiology and Cardiovascular Research, 9(2), 47-53. https://doi.org/10.11648/j.ccr.20250902.12
ACS Style
Gaye, N. D.; Ngaide, A. A.; Ngoulla, P.; Mingou, J.; Dioum, M., et al. In-Hospital Mortality of Acute Coronary Syndromes Undergoing Coronary Angiography: A Multicenter Study in Dakar, Senegal. Cardiol. Cardiovasc. Res. 2025, 9(2), 47-53. doi: 10.11648/j.ccr.20250902.12
AMA Style
Gaye ND, Ngaide AA, Ngoulla P, Mingou J, Dioum M, et al. In-Hospital Mortality of Acute Coronary Syndromes Undergoing Coronary Angiography: A Multicenter Study in Dakar, Senegal. Cardiol Cardiovasc Res. 2025;9(2):47-53. doi: 10.11648/j.ccr.20250902.12
@article{10.11648/j.ccr.20250902.12,
author = {Ngone Diaba Gaye and Aliou Alassane Ngaide and Pierre-Adley Ngoulla and Joseph Mingou and Momar Dioum and Mouhamed Chérif Mboup and Fatou Aw and Alassane Mbaye and Bamba Ndiaye and Maboury Diaw and Abdoul Kane},
title = {In-Hospital Mortality of Acute Coronary Syndromes Undergoing Coronary Angiography: A Multicenter Study in Dakar, Senegal
},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {2},
pages = {47-53},
doi = {10.11648/j.ccr.20250902.12},
url = {https://doi.org/10.11648/j.ccr.20250902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250902.12},
abstract = {Acute Coronary Syndrome (ACS) significantly contributes to cardiovascular mortality worldwide, with an increasing prevalence in Africa due to rising cardiovascular risk factors. Despite advances in reperfusion therapies like percutaneous coronary intervention (PCI), many African countries, including Senegal, face substantial barriers to optimal care. This study aimed to assess in-hospital mortality among ACS patients undergoing coronary angiography in Dakar, Senegal, and to describe clinical features associated with mortality. We conducted a retrospective, multicenter, cross-sectional study involving patients hospitalized with ACS who underwent coronary angiography between January 2020 and June 2023 in three tertiary cardiology centers in Dakar. Demographic data, clinical presentation, cardiovascular risk factors, angiographic findings, and therapeutic interventions were collected. Statistical analysis included descriptive statistics and bivariate comparisons, with significance defined at p<0.05. Out of 2573 ACS patients undergoing coronary angiography, 30 died, resulting in an in-hospital mortality rate of 1.16%. The mean age was 61.2 ± 10.8 years, predominantly male (76.7%). Hypertension (53.3%) and sedentary lifestyle (83.3%) were common risk factors. Most patients presented with atypical chest pain (76.7%) and delayed hospital admission beyond 12 hours (43.3%). STEMI accounted for 70% of cases, with the left anterior descending artery frequently involved (80%). PCI using drug-eluting stents was performed in 56.7% of deceased patients. Cardiogenic shock was the leading complication (46.7%). In-hospital mortality following coronary angiography for ACS in urban Senegal is relatively low but delayed presentations and atypical symptoms remain significant barriers. Enhanced public awareness, reduced delays to intervention, and overcoming socioeconomic obstacles are essential to improve outcomes.
},
year = {2025}
}
TY - JOUR T1 - In-Hospital Mortality of Acute Coronary Syndromes Undergoing Coronary Angiography: A Multicenter Study in Dakar, Senegal AU - Ngone Diaba Gaye AU - Aliou Alassane Ngaide AU - Pierre-Adley Ngoulla AU - Joseph Mingou AU - Momar Dioum AU - Mouhamed Chérif Mboup AU - Fatou Aw AU - Alassane Mbaye AU - Bamba Ndiaye AU - Maboury Diaw AU - Abdoul Kane Y1 - 2025/05/14 PY - 2025 N1 - https://doi.org/10.11648/j.ccr.20250902.12 DO - 10.11648/j.ccr.20250902.12 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 47 EP - 53 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20250902.12 AB - Acute Coronary Syndrome (ACS) significantly contributes to cardiovascular mortality worldwide, with an increasing prevalence in Africa due to rising cardiovascular risk factors. Despite advances in reperfusion therapies like percutaneous coronary intervention (PCI), many African countries, including Senegal, face substantial barriers to optimal care. This study aimed to assess in-hospital mortality among ACS patients undergoing coronary angiography in Dakar, Senegal, and to describe clinical features associated with mortality. We conducted a retrospective, multicenter, cross-sectional study involving patients hospitalized with ACS who underwent coronary angiography between January 2020 and June 2023 in three tertiary cardiology centers in Dakar. Demographic data, clinical presentation, cardiovascular risk factors, angiographic findings, and therapeutic interventions were collected. Statistical analysis included descriptive statistics and bivariate comparisons, with significance defined at p<0.05. Out of 2573 ACS patients undergoing coronary angiography, 30 died, resulting in an in-hospital mortality rate of 1.16%. The mean age was 61.2 ± 10.8 years, predominantly male (76.7%). Hypertension (53.3%) and sedentary lifestyle (83.3%) were common risk factors. Most patients presented with atypical chest pain (76.7%) and delayed hospital admission beyond 12 hours (43.3%). STEMI accounted for 70% of cases, with the left anterior descending artery frequently involved (80%). PCI using drug-eluting stents was performed in 56.7% of deceased patients. Cardiogenic shock was the leading complication (46.7%). In-hospital mortality following coronary angiography for ACS in urban Senegal is relatively low but delayed presentations and atypical symptoms remain significant barriers. Enhanced public awareness, reduced delays to intervention, and overcoming socioeconomic obstacles are essential to improve outcomes. VL - 9 IS - 2 ER -
Ibra Mamadou Wane Medical Center, Department of Cardiology, Dakar, Senegal
Department of Cardiology, Dalal Jamm Hospital, Guediawaye, Senegal;Department of Internal Medicine and Specialties, Cheikh Anta Diop University of Dakar, Dakar, Senegal
Department of Cardiology, Dalal Jamm Hospital, Guediawaye, Senegal;Department of Internal Medicine and Specialties, Cheikh Anta Diop University of Dakar, Dakar, Senegal
Department of Cardiology, Dalal Jamm Hospital, Guediawaye, Senegal;Department of Internal Medicine and Specialties, Cheikh Anta Diop University of Dakar, Dakar, Senegal
Information