Abstract
Introduction: Uremic pericarditis is a late complication of chronic kidney disease (CKD), often latently detected by echocardiography or clinically revealed by chest pain and a pericardial rub. The objective of our study was to describe the risk factors and outcome of uremic pericarditis in patients with chronic kidney failure at the Donka University Hospital. Methods: This was a cross-sectional, descriptive and analytical study conducted over a 7-month period from August 10 to March 10, 2022. All patients with a GFR ≤ 60 ml/min were included. The parameters studied were: epidemiological, clinical, and ultrasound. The Chi-square test was used for statistical analysis. Results: In 182 chronic uremic patients, uremic pericarditis was 12.63%. Pericardial friction rub was present to varying degrees in 91.30% of cases; the average clearance was 4.39. Pericarditis was observed on ultrasound in 82.60% of cases. The risk factors identified were: young age and terminal stage. All of our patients received extrarenal replacement therapy (ERP) and NSAIDs. Intensified EER resulted in complete resolution of pericarditis in 56.5%; surgical drainage in 4.4%, and 39.1% died. Conclusion: The prevalence of uremic pericarditis is relatively high. Early diagnosis and management could improve life expectancy.
Keywords
Risk Factors, Outcome, Uremic Pericarditis, Donka University Hospital
1. Introduction
Uremic pericarditis is a major complication of kidney disease occurring in patients with chronic kidney failure, either before or during dialysis treatment. It is the result of several factors, including poor vascular access and insufficient dialysis dose
| [1] | Boullit Oujda C. Uremic pericarditis: clinical presentation, risk factors and prognosis; Nephrology and therapeutics; 2022, 18(5), 432-433. https://doi.org/10.1016/j.nephro.2022.07.089 |
| [2] | MaHajji M, Kheder R, Smaoui W, Jebali H, Beji S, krid M et al. Uremic pericarditis in hemodialysis: Prevalence and predictive factors. Nephrology & therapeutics 11(2015) 291-292. |
[1, 2]
.
A real public health problem, uremic pericarditis remains one of the major complications of end-stage kidney disease (ESKD) linked to insufficient extrarenal replacement therapy
| [3] | Lazreg Y, Alaoui F, Hamdi F, Alaoui S, Boutaleb R, Elhebil M et al. Prevalence of uremic pericarditis. Nephrology & therapeutics 12(2016) 288–332. |
[3]
.
Very few studies on uremic pericarditis have been published in recent years. As a result, the true incidence of uremic pericarditis is difficult to establish and relies on the diagnostic criteria used, namely clinical symptoms and echocardiography.
In France, pericarditis in ESRD patients accounted for 5% of all dialysis patients in 1980
| [4] | Dussol B. Chronic renal failure. Rev. Prat; Paris 2005; 55: 1823-39. |
[4]
.
In Africa, in Morocco in 2017, a study conducted on 9 patients at the Mohamed VI University Hospital showed that the outcome of uremic pericarditis was favorable in 7 cases (77.7%), and deaths were observed in 2 cases (22.2%)
| [3] | Lazreg Y, Alaoui F, Hamdi F, Alaoui S, Boutaleb R, Elhebil M et al. Prevalence of uremic pericarditis. Nephrology & therapeutics 12(2016) 288–332. |
[3]
.
In Cameroon, the frequency of uremic pericarditis represented 62.9% in patients suffering from severe chronic kidney failure
| [5] | Youmbissi TJ, Kingues S, Djoumessi S, Guemthenc M, Tchemy C, Mpay L. Echocardiographic evaluation of 27 patients with chronic renal failure. Cardiologie tropical 1996; 22(87). |
[5]
.
In a study conducted in Morocco, 13 cases of pericarditis were observed (28.2%) after a follow-up of 14.7 months (1–27 months). The circumstances of discovery were clinical in 5 cases, based on electrocardiographic data in 3 cases. The discovery was incidental in 3 cases.
| [6] | Lengani A. Epidemiology of severe chronic renal failure in Burkina Faso. Health Journal 1997; 7-379. |
[6]
.
In Burkina Faso, a study conducted in the Internal Medicine Department of the Yalgado-Ouédrago National Hospital in Ouagadougou found an incidence of 31.6% in patients with end-stage renal disease
| [6] | Lengani A. Epidemiology of severe chronic renal failure in Burkina Faso. Health Journal 1997; 7-379. |
[6]
.
The frequency of uremic pericarditis has decreased thanks to the hemodialysis techniques used today. However, it still remains considerable in patients with end-stage renal disease.
Given the high frequency of uremic pericarditis in patients with chronic kidney failure;
1) The lack of previous studies on uremic pericarditis in chronic hemodialysis patients in Guinea;
2) The multiplicity of predictive factors for uremic pericarditis;
We deemed it appropriate to initiate this work to update data from the literature. The objective of our study was to describe the risk factors and outcome of uremic pericarditis in patients with chronic kidney failure at Donka University Hospital.
2. Patients and Methods
2.1. Study Type and Duration
We conducted a seven-month descriptive and analytical cross-sectional study, from August 10, 2019, to March 10, 2020.
2.2. Target Population
This study targeted all chronic hemodialysis patients monitored at the Donka National Hemodialysis Center during the study period.
2.3. Study Population
Our study focused on chronic hemodialysis patients with uremic pericarditis.
2.4. Selection Criteria
2.4.1. Inclusion Criteria
Our study included all patients with end-stage renal failure, whether on or off dialysis, aged 13 years and older, followed at the Donka National Hemodialysis Center, in whom uremic pericarditis was diagnosed clinically or by ultrasound.
2.4.2. Exclusion Criteria
This study excluded chronic hemodialysis patients not followed at the Donka National Hemodialysis Center and those receiving hemodialysis for acute renal failure.
2.5. Recruitment Method
We conducted an exhaustive recruitment of all patients meeting our selection criteria.
2.6. Study Variables
Our variables were quantitative and qualitative, categorized into epidemiological, clinical, and paraclinical data.
2.6.1. Qualitative Variables
The variables studied concerned socio-demographic aspects, clinical and paraclinical data.
(i). Sociodemographic Data
The variables studied were socio-demographic, gender, and socio-professional categories.
(ii). Clinical Data
We looked for functional signs such as dyspnoea and chest pain, specifying the semiological characteristics of the latter. Physical signs such as pericardial friction were also examined. Certain dialysis parameters were studied, such as interdialytic weight gain, vascular access and dialysis dose.
(iii). Paraclinical Data
1) Imaging:
Cardiac Doppler ultrasound: This is the key examination for assessing pericardial effusion and assessing its hemodynamic impact. Demonstrating an echo-free space between the two pericardial layers confirms its existence.
Assesses the abundance of the effusion: moderate if d ≤ 10 mm, moderate if d € [11, 19] mm, and very abundant if d ≥ 20 mm.
Looks for the presence or absence of a fibrin network.
Looks for compression of the cardiac chambers (Right ++++).
2) Chest X-ray:
This shows:
A distortion of the heart's silhouette with a triangular shape (teapot or carafe).
An overall increase in the cardiac shadow with a vascular pedicle that appears shortened.
Blurring of the cardiophrenic connection angles.
The cardiac silhouette will not be altered if the amount of fluid is less than 250 ml in adults and 125 ml in children.
A small, unilateral or bilateral pleural effusion may often be present.
(iv). Prognostic Data
1) Dialysis initiation
a) Early;
b) Late.
2) Morbidity and mortality
2.6.2. Quantitative Variables
We expressed the frequency as a percentage and divided the patients into age groups according to 10-year intervals.
We then calculated the median age and gave the extreme ages.
2.7. Data Analysis
Our data were collected manually on data sheets and analyzed using SPSS software version 21.
2.8. Analysis Plan
The descriptive study was conducted by calculating frequencies and proportions for qualitative variables, and by calculating means for quantitative variables.
The analytical study was conducted using cross-tabulations; comparisons were performed using the Chi-square test or the Fisher test when the calculated sample size was lower. The difference was considered statistically significant when the P < 0.05.
2.9. Ethical Considerations
During this study, free consent was obtained from the patient, and the anonymity of the individuals surveyed and data confidentiality were respected.
3. Results
Table 1. Distribution of patients by sociodemographic characteristics.
Variables | Number | % |
Sex |
Male | 14 | 60.87 |
Female | 9 | 39.13 |
Years |
10-19 | 3 | 13.04 |
20-29 | 5 | 21.74 |
30-39 | 5 | 21.74 |
40-49 | 4 | 17.40 |
50-59 | 3 | 13.04 |
≥60 | 3 | 13.04 |
Total | 23 | 100 |
Average age = 37.30±15.15 Sex ratio M/F: 0.64
In this table, the male sex was 60.87% and patients aged 20 to 39 years represented 43%.
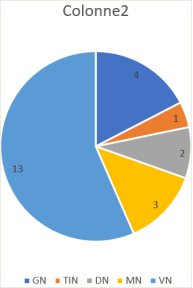
Figure 1. Distribution of patients according to initial nephropathy.
This figure shows a frequency of 56.52% of cases of vascular nephropathy and 17% of cases of glomerular nephropathy.
Table 2. Distribution of patients according to observed clinical signs.
Clinical signs | Variables | Number | % |
Functional | Dyspnea | 18 | 78.26 |
Chest pain | 20 | 86.95 |
Cough | 11 | 47.8 |
Hiccups | 4 | 17.4 |
Physical | Pericardial friction rub | 21 | 91.30 |
Ascites | 7 | 30.43 |
Hepatojugular reflux | 2 | 8.7 |
Pleurisy | 5 | 21.73 |
Hypotension | 2 | 8.7 |
Systolic murmur | 6 | 26.1 |
Hepatomegaly | 3 | 13 |
Jugular vein turgor | 7 | 30.43 |
Edema in the lower limbs | 16 | 69.6 |
This table shows the main functional signs, which were chest pain and dyspnea, with pericardial friction rub representing the most dominant physical sign in 91% of cases.
Table 3. Distribution of patients according to electrocardiogram data.
Variables | Number | % |
Electrocardiogram |
Left ventricular hypertrophy | 4 | 17.39 |
Hypertensive heart disease | 2 | 8.69 |
Microvoltage and/or repolarization disorder, tachycardia, ST segment elevation | 8 | 34.78 |
Not performed | 9 | 39.14 |
Cardiac ultrasound |
Tamponade | 2 | 8.69 |
Fluid pericarditis | 12 | 52.17 |
Dry pericarditis (thickening, calcification) | 5 | 21.74 |
Not performed | 4 | 17.4 |
Chest X-ray |
Normal X-ray | 1 | 4.35 |
Pleural effusion | 5 | 21.74 |
Not performed | 5 | 21.74 |
Table 4. Distribution according to associated factors.
Evolution |
Risk factors | Improved | Died | Total | p-value |
Male gender | 8 | 6 | 14 | 0.000 |
Young age | 4 | 6 | 10 | 0.000 |
Insufficient dialysis dose | 2 | 8 | 10 | 0.001 |
Late onset of dialysis | 2 | 6 | 8 | 0.000 |
Uremia | 14 | 7 | 21 | 0.000 |
End-stage CKD | 13 | 9 | 22 | 0.59 |
IWG˃4 | 1 | 3 | 4 | 0.000 |
Use of femoral catheter | 1 | 8 | 9 | 0.000 |
Total | 45 | 53 | 98 | |
4. Discussion
The modest sample size, the insufficient technical capacity, and the low socioeconomic status of the patients were limitations of this study.
Despite these shortcomings, the results obtained allowed us to achieve our objectives.
Very few studies on uremic pericarditis have been published in recent years, and the majority of them do not address prognostic factors.
In our series, we recorded 23 chronic hemodialysis patients diagnosed with pericarditis out of a total of 182 chronic hemodialysis patients surveyed, representing a prevalence of 12.63%.
Our results are higher than those of Aloui A. et al in Tunisia, Ezziani M. et al in Morocco and Masson JF. et al. in France who found a respective prevalence of 7.9%, 6% and 9.25%
| [7] | Aloui A, Chargui S, Ladhari N, Younsi F, Ben Abdallah T. Pericarditis in terminal chronic renal failure. Nephrology & Therapeutics; 2016: 12(5), 315. |
| [8] | M Ezziani et al. Ultrasound abnormalities in chronic hemodialysis patients: prevalence and risk factors. Pan African medical journal. 2014. Available at:
https://doi.org/10.11604/pamj.2014.18.216.4438 |
| [9] | Masson JF, Maes ML, Zilberman C. Pericarditis in chronic renal failure patients treated by periodic hemodialysis. Internal Medicine Review. 1981, Volume II, Vol 4: 447–453. |
[7-9]
. This high prevalence in our series is undoubtedly linked to irregular patient follow-up or late nephrological management, insufficient weekly hemodialysis duration (less than 12 hours), reasons for vascular access dysfunction and significant inter-dialytic weight gain.
1) The mean age of our patients was 37.30±15.15 years with extremes of 13 years and 65 years. Patients with uremic pericarditis were more represented in the 20-39 age group (10 patients or 43.48%) followed by the 40-49 age group (4 patients or 17.40%). This was therefore a relatively young population, similar to the data of Boukari Bako Bibata in Mali
| [2] | MaHajji M, Kheder R, Smaoui W, Jebali H, Beji S, krid M et al. Uremic pericarditis in hemodialysis: Prevalence and predictive factors. Nephrology & therapeutics 11(2015) 291-292. |
[2]
. In the United States, Srikanth Yandrapalli et al found an average age of 55 years for patients
| [10] | Yandarpalli et al. Prevalence and in-hospital outcomes of uremic and dialysis pericarditis: a united state national study. Journal of the American College of Cardiology. 2017; 69(11): 1743. |
[10]
. The average age of our patients was lower than those observed in the West; this could be explained by a much younger population in Guinea. The increase in life expectancy of hemodialysis patients in the West could explain this age difference. In our study there was a male predominance with a sex ratio of 0.64, which is consistent with the data of A. Aliou et al in Tunisia
| [6] | Lengani A. Epidemiology of severe chronic renal failure in Burkina Faso. Health Journal 1997; 7-379. |
[6]
. This result is contrary to that of Aneediya Bederji of London where the female sex was predominant (60% versus 40% male)
| [11] | Banerjee A, Davenport A. Altered patterns of pericardial disease in patients with end-stage renal disease. Hemodialysis International 2006; 10: 249–255. |
[11]
. This male predominance could be explained by the fact that men are more exposed to other risk factors than women such as smoking, stress, alcoholism which can lead them to high blood pressure in the long term, which is one of the causes of renal failure.
2) Vascular nephropathy represented the most frequent initial nephropathy in our series 56.52%. This result is contrary to that reported by Y. Lazreg in Rabat and S. Amor in Tunisia where the initial nephropathy was dominated by glomerular and interstitial nephropathy
| [3] | Lazreg Y, Alaoui F, Hamdi F, Alaoui S, Boutaleb R, Elhebil M et al. Prevalence of uremic pericarditis. Nephrology & therapeutics 12(2016) 288–332. |
| [12] | Amor S et al. Ultrasound abnormalities found in patients on chronic hemodialysis. Nephrology and Therapeutics 11 (2015) 287–337. |
[3, 12]
. This difference could also probably be explained by the absence of early and regular management of hypertension and the higher frequency of hypertensive disease in black African subjects.
Pericardial rub, a pathognomonic sign of the condition, was present in 21 patients (91.30%) to varying degrees. Chest pain, the second most common clinical manifestation in our study, was present in 20 patients (86.95%).
This frequency is consistent with that observed in the literature
| [14] | Taimur D, Mark JS. Pericarditis and pericardial effusions in end-stage renal disease. Division of Nephrology, Tufts Medical Center, 2016. Available at: https://doi.org/10.1111/sdi.1217 |
| [15] | Yassamine B, Hamdi F, Chemlal A, Haddiya I, Ismaili N, El Ouafi N. Uremic pericarditis in patients with end-stage renal disease: Prevalence, symptoms, and outcomes in 2017. Yajem 57118. Available at:
https://doi.org/10.1016/j.ajem.2017.11.048 |
[14, 15]
. Pericardial rub and/or chest pain dominate the presentation of pericarditis
| [2] | MaHajji M, Kheder R, Smaoui W, Jebali H, Beji S, krid M et al. Uremic pericarditis in hemodialysis: Prevalence and predictive factors. Nephrology & therapeutics 11(2015) 291-292. |
| [13] | Morin JE, Hollomby D, Gonda A, Long R, Dobell ARC. Management of uremic pericarditis: a report of 11 patients with cardiac tamponade. Annals of Thoracic Surgery. 1976; vol. 22: 588-591. |
| [15] | Yassamine B, Hamdi F, Chemlal A, Haddiya I, Ismaili N, El Ouafi N. Uremic pericarditis in patients with end-stage renal disease: Prevalence, symptoms, and outcomes in 2017. Yajem 57118. Available at:
https://doi.org/10.1016/j.ajem.2017.11.048 |
| [16] | Karim AR et al. Uremic pericarditis, pericardial effusion, and constrictive pericarditis in end-stage renal disease: Insights and pathophysiology. Clinical Cardiology. 2017; 40: 839-846. |
[2, 13, 15, 16]
. It should be noted that pericardial rub is not consistently found in all patients with pericarditis, hence the importance of echocardiography in the diagnosis of pericarditis.
The absence of pericardial rub in 2 patients (8.69%) should be noted, as well as its association with a state of extracellular hyperhydration: lower limb edema (16 cases), ascites (7 cases), and pleurisy (5 cases). Clinical signs of right heart failure were found in some patients, in unequal proportions: hepatomegaly (3 cases), hepatojugular reflux (2 cases), jugular distension (7 cases), systolic murmur (6 cases). Hypotension, a sign of acute decompensation, was found in 2 patients.
Signs of mediastinal distress such as cough and hiccups were found in 11 and 4 patients, respectively. The clinical manifestations in our study are comparable to those reported in the literature
| [13] | Morin JE, Hollomby D, Gonda A, Long R, Dobell ARC. Management of uremic pericarditis: a report of 11 patients with cardiac tamponade. Annals of Thoracic Surgery. 1976; vol. 22: 588-591. |
| [15] | Yassamine B, Hamdi F, Chemlal A, Haddiya I, Ismaili N, El Ouafi N. Uremic pericarditis in patients with end-stage renal disease: Prevalence, symptoms, and outcomes in 2017. Yajem 57118. Available at:
https://doi.org/10.1016/j.ajem.2017.11.048 |
[13, 15]
.
Echocardiography is the diagnostic procedure of choice if acute pericarditis is suspected
| [14] | Taimur D, Mark JS. Pericarditis and pericardial effusions in end-stage renal disease. Division of Nephrology, Tufts Medical Center, 2016. Available at: https://doi.org/10.1111/sdi.1217 |
| [17] | Maoud F. Pericarditis in chronic dialysis patients: a report of 5 cases. Medical thesis. Rabat: Mohammed V University, 2016; (4-7 p). |
[14, 17]
. Indeed, it allows confirmation and monitoring of the development of pericardial effusion and its impact on cardiac function, sometimes guiding etiological investigations
| [14] | Taimur D, Mark JS. Pericarditis and pericardial effusions in end-stage renal disease. Division of Nephrology, Tufts Medical Center, 2016. Available at: https://doi.org/10.1111/sdi.1217 |
[14]
. Pericarditis was observed on ultrasound in our series in 19 patients (82.60%) or 52.17% for pericardial effusions (7 of small abundance, 5 of medium abundance), 21.74% for dry pericarditis and 8.69% for tamponades. Left ventricular hypertrophy is also particularly common. It is thought to be multifactorial: anemia, dialysis, and hypertension.
Of 18 standard chest X-rays performed, 17 patients had abnormalities, 12 of which showed an enlarged cardiac silhouette.
In our study, we did not find a statistically significant link between end-stage renal disease and uremic pericarditis (P=0.59). After cross-referencing risk factors for uremic pericarditis with the progression of our patients' condition, we found statistically significant links (P=0.000) between insufficient dialysis dose, use of a femoral catheter, young age, significant inter-dialysis weight gain, male gender, and the occurrence of uremic pericarditis. This could call into question the fact that uremic pericarditis always appears in the end-stage of kidney disease. However, end-stage renal disease remains a classic risk factor for pericarditis in chronic hemodialysis patients. Risk factors vary from one study to another and also depend on the parameters studied. Thus, in the study by Hajji M
| [2] | MaHajji M, Kheder R, Smaoui W, Jebali H, Beji S, krid M et al. Uremic pericarditis in hemodialysis: Prevalence and predictive factors. Nephrology & therapeutics 11(2015) 291-292. |
[2]
, in multivariate analysis, the parameters identified as independent factors associated with the occurrence of pericarditis were: a percentage reduction in urea < 40% (p = 0.004), the use of femoral silencing (p = 0.01), an interdialytic weight gain > 4 kg (p = 0.003) and the number of sessions < 3/week (p = 0.001).
5. Conclusion
Despite the hemodialysis techniques used today, the prevalence of uremic pericarditis remains high in our hemodialysis center.
Insufficient dialysis dose, late dialysis, use of a femoral catheter, and end-stage chronic renal failure were the risk factors associated with the occurrence of uremic pericarditis.
A longitudinal study including systematic cardiac ultrasound would allow for early diagnosis of latent forms of uremic pericarditis to ensure appropriate management.
Abbreviations
GN | Glomerular Nephropathy |
VN | Vascular Nephropathy |
TUN | Tubulunterstitial Nephropathy |
DN | Diabetic Nephropathy |
MN | Mixed Nephropathy |
IWG | Interdialytic Weight Gain |
Acknowledgments
The authors thank the cardiologists who performed these examinations.
Author Contributions
Fousseny Diakite: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Kadiatou Mamadou Bobo Barry: Methodology, Supervision, Validation, Visualization, Writing – original draft.
Ibrahima Sory Barry: Methodology, Supervision, Validation, Visualization, Writing – review & editing.
Aly Traore: Methodology, Supervision, Validation, Visualization.
Doussou Kaba: Validation, Visualization.
Mariame Komah: Supervision, Validation, Visualization.
Aminata 1 Diallo: Validation, Visualization.
Soriba Bangoura: Validation, Visualization.
Mohamed Lamine Tegui Camara: Validation, Visualization.
Damaris Yawa Leno: Validation, Visualization.
Mohamed Lamine Kaba: investigation.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Boullit Oujda C. Uremic pericarditis: clinical presentation, risk factors and prognosis; Nephrology and therapeutics; 2022, 18(5), 432-433.
https://doi.org/10.1016/j.nephro.2022.07.089
|
| [2] |
MaHajji M, Kheder R, Smaoui W, Jebali H, Beji S, krid M et al. Uremic pericarditis in hemodialysis: Prevalence and predictive factors. Nephrology & therapeutics 11(2015) 291-292.
|
| [3] |
Lazreg Y, Alaoui F, Hamdi F, Alaoui S, Boutaleb R, Elhebil M et al. Prevalence of uremic pericarditis. Nephrology & therapeutics 12(2016) 288–332.
|
| [4] |
Dussol B. Chronic renal failure. Rev. Prat; Paris 2005; 55: 1823-39.
|
| [5] |
Youmbissi TJ, Kingues S, Djoumessi S, Guemthenc M, Tchemy C, Mpay L. Echocardiographic evaluation of 27 patients with chronic renal failure. Cardiologie tropical 1996; 22(87).
|
| [6] |
Lengani A. Epidemiology of severe chronic renal failure in Burkina Faso. Health Journal 1997; 7-379.
|
| [7] |
Aloui A, Chargui S, Ladhari N, Younsi F, Ben Abdallah T. Pericarditis in terminal chronic renal failure. Nephrology & Therapeutics; 2016: 12(5), 315.
|
| [8] |
M Ezziani et al. Ultrasound abnormalities in chronic hemodialysis patients: prevalence and risk factors. Pan African medical journal. 2014. Available at:
https://doi.org/10.11604/pamj.2014.18.216.4438
|
| [9] |
Masson JF, Maes ML, Zilberman C. Pericarditis in chronic renal failure patients treated by periodic hemodialysis. Internal Medicine Review. 1981, Volume II, Vol 4: 447–453.
|
| [10] |
Yandarpalli et al. Prevalence and in-hospital outcomes of uremic and dialysis pericarditis: a united state national study. Journal of the American College of Cardiology. 2017; 69(11): 1743.
|
| [11] |
Banerjee A, Davenport A. Altered patterns of pericardial disease in patients with end-stage renal disease. Hemodialysis International 2006; 10: 249–255.
|
| [12] |
Amor S et al. Ultrasound abnormalities found in patients on chronic hemodialysis. Nephrology and Therapeutics 11 (2015) 287–337.
|
| [13] |
Morin JE, Hollomby D, Gonda A, Long R, Dobell ARC. Management of uremic pericarditis: a report of 11 patients with cardiac tamponade. Annals of Thoracic Surgery. 1976; vol. 22: 588-591.
|
| [14] |
Taimur D, Mark JS. Pericarditis and pericardial effusions in end-stage renal disease. Division of Nephrology, Tufts Medical Center, 2016. Available at:
https://doi.org/10.1111/sdi.1217
|
| [15] |
Yassamine B, Hamdi F, Chemlal A, Haddiya I, Ismaili N, El Ouafi N. Uremic pericarditis in patients with end-stage renal disease: Prevalence, symptoms, and outcomes in 2017. Yajem 57118. Available at:
https://doi.org/10.1016/j.ajem.2017.11.048
|
| [16] |
Karim AR et al. Uremic pericarditis, pericardial effusion, and constrictive pericarditis in end-stage renal disease: Insights and pathophysiology. Clinical Cardiology. 2017; 40: 839-846.
|
| [17] |
Maoud F. Pericarditis in chronic dialysis patients: a report of 5 cases. Medical thesis. Rabat: Mohammed V University, 2016; (4-7 p).
|
Cite This Article
-
APA Style
Diakite, F., Barry, K. M. B., Barry, I. S., Traore, A., Kaba, D., et al. (2026). Risk Factors and Outcome of Uremic Pericarditis in Patients with Chronic Kidney Failure at Donka University Hospital. Cardiology and Cardiovascular Research, 10(1), 1-6. https://doi.org/10.11648/j.ccr.20261001.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Diakite, F.; Barry, K. M. B.; Barry, I. S.; Traore, A.; Kaba, D., et al. Risk Factors and Outcome of Uremic Pericarditis in Patients with Chronic Kidney Failure at Donka University Hospital. Cardiol. Cardiovasc. Res. 2026, 10(1), 1-6. doi: 10.11648/j.ccr.20261001.11
Copy
|
Download
AMA Style
Diakite F, Barry KMB, Barry IS, Traore A, Kaba D, et al. Risk Factors and Outcome of Uremic Pericarditis in Patients with Chronic Kidney Failure at Donka University Hospital. Cardiol Cardiovasc Res. 2026;10(1):1-6. doi: 10.11648/j.ccr.20261001.11
Copy
|
Download
-
@article{10.11648/j.ccr.20261001.11,
author = {Fousseny Diakite and Kadiatou Mamadou Bobo Barry and Ibrahima Sory Barry and Aly Traore and Doussou Kaba and Mariame Komah and Aminata 1 Diallo and Soriba Bangoura and Mohamed Lamine Tegui Camara and Damaris Yawa Leno and Mohamed Lamine Kaba},
title = {Risk Factors and Outcome of Uremic Pericarditis in Patients with Chronic Kidney Failure at Donka University Hospital},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {1},
pages = {1-6},
doi = {10.11648/j.ccr.20261001.11},
url = {https://doi.org/10.11648/j.ccr.20261001.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261001.11},
abstract = {Introduction: Uremic pericarditis is a late complication of chronic kidney disease (CKD), often latently detected by echocardiography or clinically revealed by chest pain and a pericardial rub. The objective of our study was to describe the risk factors and outcome of uremic pericarditis in patients with chronic kidney failure at the Donka University Hospital. Methods: This was a cross-sectional, descriptive and analytical study conducted over a 7-month period from August 10 to March 10, 2022. All patients with a GFR ≤ 60 ml/min were included. The parameters studied were: epidemiological, clinical, and ultrasound. The Chi-square test was used for statistical analysis. Results: In 182 chronic uremic patients, uremic pericarditis was 12.63%. Pericardial friction rub was present to varying degrees in 91.30% of cases; the average clearance was 4.39. Pericarditis was observed on ultrasound in 82.60% of cases. The risk factors identified were: young age and terminal stage. All of our patients received extrarenal replacement therapy (ERP) and NSAIDs. Intensified EER resulted in complete resolution of pericarditis in 56.5%; surgical drainage in 4.4%, and 39.1% died. Conclusion: The prevalence of uremic pericarditis is relatively high. Early diagnosis and management could improve life expectancy.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Risk Factors and Outcome of Uremic Pericarditis in Patients with Chronic Kidney Failure at Donka University Hospital
AU - Fousseny Diakite
AU - Kadiatou Mamadou Bobo Barry
AU - Ibrahima Sory Barry
AU - Aly Traore
AU - Doussou Kaba
AU - Mariame Komah
AU - Aminata 1 Diallo
AU - Soriba Bangoura
AU - Mohamed Lamine Tegui Camara
AU - Damaris Yawa Leno
AU - Mohamed Lamine Kaba
Y1 - 2026/02/11
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261001.11
DO - 10.11648/j.ccr.20261001.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 1
EP - 6
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261001.11
AB - Introduction: Uremic pericarditis is a late complication of chronic kidney disease (CKD), often latently detected by echocardiography or clinically revealed by chest pain and a pericardial rub. The objective of our study was to describe the risk factors and outcome of uremic pericarditis in patients with chronic kidney failure at the Donka University Hospital. Methods: This was a cross-sectional, descriptive and analytical study conducted over a 7-month period from August 10 to March 10, 2022. All patients with a GFR ≤ 60 ml/min were included. The parameters studied were: epidemiological, clinical, and ultrasound. The Chi-square test was used for statistical analysis. Results: In 182 chronic uremic patients, uremic pericarditis was 12.63%. Pericardial friction rub was present to varying degrees in 91.30% of cases; the average clearance was 4.39. Pericarditis was observed on ultrasound in 82.60% of cases. The risk factors identified were: young age and terminal stage. All of our patients received extrarenal replacement therapy (ERP) and NSAIDs. Intensified EER resulted in complete resolution of pericarditis in 56.5%; surgical drainage in 4.4%, and 39.1% died. Conclusion: The prevalence of uremic pericarditis is relatively high. Early diagnosis and management could improve life expectancy.
VL - 10
IS - 1
ER -
Copy
|
Download